





Best Formula for GERD in Infants With Persistent Reflux Symptoms

You’ve just changed your baby’s outfit for the third time today after another round of spit-up. Your baby arches their back during feedings, refuses the bottle halfway through, and wakes up crying multiple times each night. At your last visit, the pediatrician mentioned reflux, and now you’re wondering if switching formulas might help.
When a pediatrician brings up reflux, it’s natural to wonder how serious it might be. Studies show that 37.8% of regurgitant infants (babies who spit up frequently) experience gastroesophageal reflux disease (GERD). If your doctor has mentioned GERD, you’re likely searching for answers about which formula might ease your baby’s discomfort.
This guide will walk you through what reflux and GERD actually mean, when formula changes make sense, and what types of formulas doctors typically consider for babies with confirmed reflux. Understanding these options can help you have better conversations with your pediatrician about what might work for your baby.
Key Takeaways
- Most infant spit-up is normal and does not require treatment or formula changes.
- GERD is diagnosed when reflux causes pain, feeding refusal, or poor weight gain.
- Formula changes for GERD are made only when medically indicated, often due to intolerance or allergy.
- Thickened, extensively hydrolyzed, or amino acid–based formulas are chosen based on the cause of symptoms.
- Specialty formulas may be medically necessary and can sometimes be covered by insurance with proper documentation.
Is It Normal for Babies to Spit Up?

Yes. Spitting up is very common in infants, especially during the first few months of life. In most cases, it is a normal part of development and not a sign of illness.
Infants have an immature digestive system. The muscle that keeps food in the stomach, the lower esophageal sphincter, is still developing, which makes it easier for milk to flow back into the esophagus after feeding. This is often referred to as infant reflux.
Many babies spit up:
- After feeding
- When burped
- When lying flat shortly after eating
If a baby is feeding well, gaining weight appropriately, and generally comfortable, spitting up is usually harmless. Pediatricians often refer to these infants as “happy spitters.” In such cases, treatment or formula changes are typically not necessary.
It is important to note that spit-up can be misleading. Even a small amount of milk can look like a lot when it soaks into clothes or sheets.
Spitting up becomes more concerning when it is frequent, persistent, or associated with other symptoms, such as poor weight gain, feeding refusal, or signs of discomfort. These situations may require further evaluation, which is discussed in later sections.
Spit-Up vs Reflux vs GERD in Infants
Spitting up is often described using different terms, which can be confusing for parents. While these terms are related, they do not all mean the same thing. Understanding the differences can help clarify when symptoms are normal and when medical evaluation may be needed.
Key Differences at a Glance
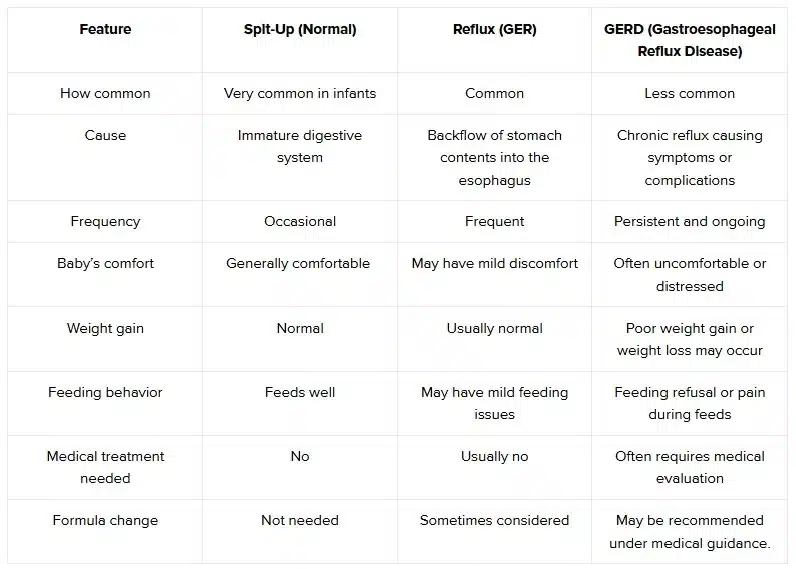
Most infants who spit up fall into the normal spit-up or mild reflux (GER) category and improve as their digestive system matures. In these cases, reassurance and simple feeding adjustments are often sufficient.
GERD is different. It is diagnosed when reflux is persistent and interferes with feeding, growth, or comfort. This distinction is important because GERD may require a more structured approach to diagnosis and treatment, including careful consideration of feeding strategies and, in some cases, formula changes.
Note: GERD and cow’s milk protein allergy can look very similar. Some babies may have one condition, both, or neither. Your pediatrician will help figure out what’s actually causing your baby’s symptoms.
Suggested Read: A New Parent’s Guide To Cluster Feeding
Common Symptoms of Infant Reflux and GERD

GERD symptoms in babies can vary widely and often look similar to other conditions. This is why a thorough checkup by your pediatrician is essential for proper diagnosis.
Common signs that may point to GERD include:
- Frequent or forceful vomiting beyond typical spit-up.
- Crying, fussiness, or arching during or right after feedings.
- Refusing to eat or pulling away from the bottle or breast.
- Poor weight gain or failure to meet growth milestones.
- Chronic cough, wheezing, or repeated respiratory issues.
- Sleep problems due to apparent discomfort.
- Difficulty swallowing.
If your baby shows several of these symptoms regularly, your pediatrician may investigate whether the formula type, feeding technique, or an underlying medical issue is contributing to the problem.
It’s important to know that not all crying or fussiness in babies is related to GERD. Many other factors can cause similar behaviors, which is why a medical evaluation matters before making changes to your baby’s feeding routine.
What Causes Reflux in Infants?
Infant reflux occurs primarily because a baby’s digestive system is still developing. In most cases, it is not caused by illness and improves naturally as the baby grows.
One of the main contributors is an immature lower esophageal sphincter, the muscle that separates the esophagus from the stomach. In young infants, this muscle may relax more easily, allowing stomach contents to flow back into the esophagus after feeding.
Other common factors that can contribute to reflux include:
- Liquid-only diet: Milk moves more easily back into the esophagus than solid food.
- Lying flat after feeds: Gravity helps keep milk in the stomach.
- Overfeeding: Large feeding volumes can increase gastric pressure.
- Swallowing air during feeds: This can increase gastric pressure and lead to spit-up.
In some infants, reflux symptoms may be worsened by feeding intolerance rather than the reflux itself. This can occur when a baby has difficulty digesting certain formula proteins or has an underlying sensitivity, such as a cow’s milk protein allergy. In these cases, reflux-like symptoms may persist despite typical feeding adjustments.
It is also important to understand that reflux can have multiple contributing factors. For example, an infant may have both an immature digestive system and a sensitivity to certain formula ingredients. Identifying the underlying cause helps guide appropriate management and determines whether changes in feeding approach or formula may be considered.
Suggested Read: Comfortable Breastfeeding Positions You Can Try
When Do Doctors Consider Changing the Formula for Reflux?

A change in formula is usually considered only when reflux symptoms suggest an underlying medical or feeding issue, rather than normal infant reflux.
Pediatricians may consider a formula change when:
- Reflux symptoms are persistent and severe.
- Feeding appears painful or consistently distressing.
- An infant shows poor weight gain or weight loss.
- Symptoms do not improve with standard feeding and positioning adjustments.
- There is concern for cow’s milk protein allergy or other intolerance.
In these situations, a formula change is not used as a trial-and-error approach, but as a targeted response based on the infant’s symptoms, growth pattern, and medical history.
Before recommending a change, healthcare providers often review:
- Feeding volume and frequency.
- Growth trends.
- Associated symptoms such as diarrhea, blood in stools, or eczema.
This careful assessment helps ensure that any formula change addresses a specific clinical concern rather than introducing unnecessary dietary changes.
Types of Formula Commonly Used for Infants With Reflux

When formula changes are medically appropriate, there are several types that pediatricians may consider based on your baby’s specific symptoms and diagnosis.
Thickened (Anti-Reflux) Formulas
Thickened formulas are designed to make feeds heavier, which can help reduce the likelihood of milk flowing back into the esophagus after feeding. This approach focuses on reducing visible spit-up, rather than addressing digestion or allergy.
These formulas are usually discussed when:
- Your baby spits up frequently but seems otherwise comfortable.
- Weight gain is appropriate.
- There are no signs of milk protein allergy or intolerance.
In the U.S., pediatricians often use options like Enfamil A.R. or Similac for Spit-Up for this purpose. Because these formulas are thicker, your baby may need a nipple with a slightly larger opening to keep feeds comfortable and steady.
While thickened formulas can reduce spit-up, they do not address all reflux-related symptoms and are typically used under your pediatrician’s guidance.
Extensively Hydrolyzed Formulas
When reflux symptoms are accompanied by feeding discomfort or ongoing digestive issues, your pediatrician may consider whether cow’s milk protein sensitivity is playing a role. Extensively hydrolyzed formulas are designed to improve tolerance by breaking proteins into much smaller fragments.
This type of formula is often considered when reflux occurs along with:
- Ongoing fussiness during feeds.
- Gastrointestinal symptoms beyond spit-up.
- Signs suggestive of milk protein allergy.
Formulas such as Nutramigen, Similac Alimentum, or Pregestimil are commonly used in these situations. These formulas can taste different from standard formulas, and it may take 1 to 4 weeks to see whether symptoms improve.
If reflux and feeding discomfort lessen over time, it can indicate that protein sensitivity was contributing to your baby’s symptoms.
Amino Acid–Based Formulas
Amino acid–based formulas are used in more complex cases, especially when symptoms persist despite other feeding changes or when a more severe allergy is suspected.
Instead of protein fragments, these formulas provide nutrition as individual amino acids, greatly reducing the risk of triggering an allergic response.
They are typically considered when:
- Symptoms remain significant despite other formula changes.
- A severe or multiple food allergy is suspected or confirmed.
- Feeding difficulties begin to affect growth or comfort.
Options such as Neocate, EleCare, or PurAmino are commonly prescribed in these cases. Because these formulas are highly specialized and more expensive, they are usually introduced with close medical supervision.
What Formula Alone Cannot Fix?

It’s important to have realistic expectations about what changing the formula can and cannot do.
Formula changes work best when symptoms are related to a food allergy or sensitivity. However, GERD caused purely by an immature valve between the food pipe and stomach may not improve significantly with formula changes alone.
Formula Won’t Address:
- Physical issues like a significant hiatal hernia.
- Severe complications in the food pipe that require medical treatment.
- All crying and fussiness (many babies cry for reasons unrelated to feeding).
- The natural development timeline of the valve that prevents reflux.
What May Still Be Needed:
Some babies require a combination approach that might include formula changes, adjustments to feeding techniques, keeping the baby upright after feeds, or, in some cases, medication prescribed by a pediatrician. The severity of GERD and the cause will determine the best treatment path.
Your pediatrician can help set appropriate expectations based on your baby’s specific situation and track whether the current approach is working.
Suggested Read: Prenatal Vitamins Explained: Finding the Best Formula with Folic Acid
How to Treat Infant Reflux Safely?

Feeding and nutrition changes are recommended as a first approach in babies before considering other treatments.
Initial strategies your pediatrician may recommend include:
Feeding Changes
- Offering smaller, more frequent feedings to reduce stomach volume.
- Make sure the bottle is positioned properly to minimize air swallowing.
- Keeping your baby upright for 20 to 30 minutes after feeding.
- Burping frequently during feedings.
Formula Considerations
If cow’s milk protein sensitivity is suspected, a trial of extensively hydrolyzed formula for 2 to 4 weeks may be suggested. If your baby shows improvement during this trial period, it helps confirm that the formula type was part of the issue.
When Medication May Be Considered
For babies with confirmed GERD who don’t respond to feeding changes, your pediatrician may discuss medications that reduce stomach acid secretion. However, these are not routinely recommended for all babies with reflux and should be carefully considered. Common options include Nexium (esomeprazole), Prevacid (lansoprazole), and Pepcid (famotidine).
What Doesn’t Help
Current evidence doesn’t support the use of probiotics, gripe water, or many other over-the-counter remedies specifically for GERD. Always discuss any supplements or alternative treatments with your pediatrician before trying them.
The good news is that most cases of infant reflux get better by 6 to 12 months of age as the valve between the food pipe and stomach matures and babies spend more time sitting upright.
When to Talk to Your Pediatrician
Schedule an appointment with your baby’s doctor if you notice:
- Spit-up that seems forceful or shoots out (projectile vomiting).
- Refusing to eat or a significant drop in interest in feeding.
- Blood in spit-up or stool.
- Poor weight gain or weight loss.
- Persistent crying or signs of pain during or after feedings.
- Breathing problems, chronic cough, or wheezing.
- Symptoms that interfere with daily life despite trying standard reflux management strategies.
Don’t wait; if you see warning signs like bile (green or yellow liquid) in vomit, severe sleepiness, or signs of dehydration. These require immediate medical attention.
Trust your instincts as a parent. If something feels wrong or your baby’s symptoms are affecting their quality of life or yours, it’s worth having a conversation with your pediatrician, even if you’re not sure whether it’s serious enough.
Conclusion
Finding the best formula for GERD in infants is rarely about picking a product from a list. It is about understanding your baby’s individual needs and knowing when extra support is truly necessary. For some babies, a specific formula can improve feeding comfort and reduce symptoms. For others, time, growth, and simple feeding adjustments play an equally important role. What matters most is feeling informed, supported, and confident as you move forward.
If your pediatrician has determined that a specialty formula is medically necessary, access and affordability should not add to the stress you are already experiencing. This is where Insurance Covered Baby Formula can help. At Insurance Covered Baby Formula, our team supports families by exploring whether their insurance plan may cover prescribed formulas and by helping with the required documentation, so you can focus your energy on caring for your baby.
You do not have to navigate this alone. If your baby has been diagnosed with GERD and a specialized formula has been recommended, reach out to us today. Our team is here to help you understand your options and take the next step with clarity, care, and compassion.
FAQs
1. Is GERD more common in formula-fed babies?
GERD is not proven to be more common in formula-fed babies; feeding volume, technique, and individual sensitivity matter more than breast versus formula feeding.
2. How can you tell if a newborn has GERD?
Newborn GERD is suspected when reflux causes pain, feeding refusal, poor weight gain, breathing symptoms, or sleep disruption, and should be evaluated by a pediatrician.
3. Is reflux caused by overfeeding?
Overfeeding can worsen reflux by increasing stomach pressure, but reflux also occurs with normal feeds due to immature digestion, positioning, or swallowed air.
4. What are the signs of an overfed baby?
Signs of overfeeding include frequent spit-up, vomiting, fussiness after feeds, gassiness, loose stools, fast weight gain, and discomfort relieved by smaller, paced feedings.
5. Is reflux a risk factor for SIDS?
Reflux is not considered a risk factor for SIDS; placing babies on their backs to sleep remains safe and recommended, even for infants with reflux.